














 " alt="">
" alt="">


























Executive Insights
Alex Lirtsman
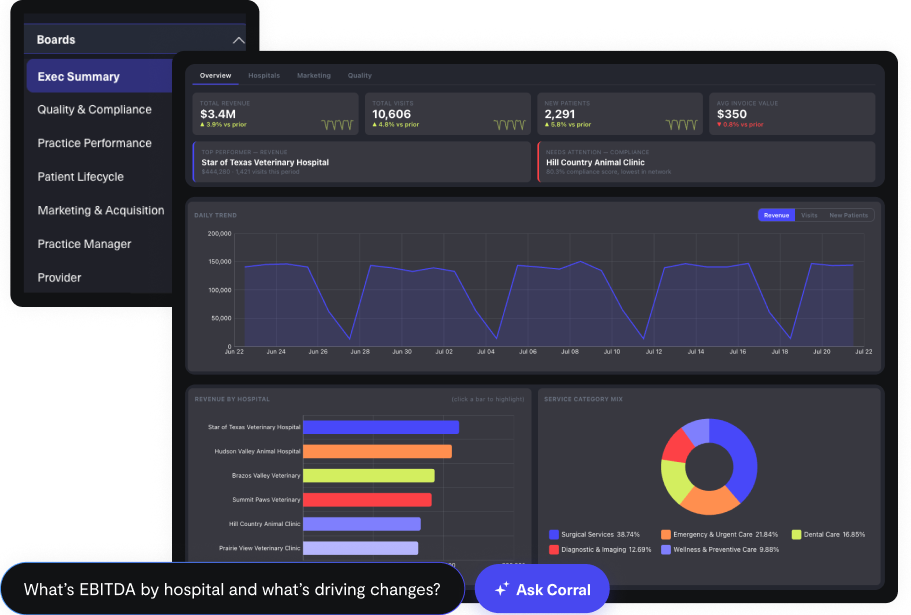
Use AI to effortlessly answer any business questions from all your data.
CorralData MCP brings your business data and intelligence directly into Claude and other AI assistants
Build and share custom data applications powered by your connected data.
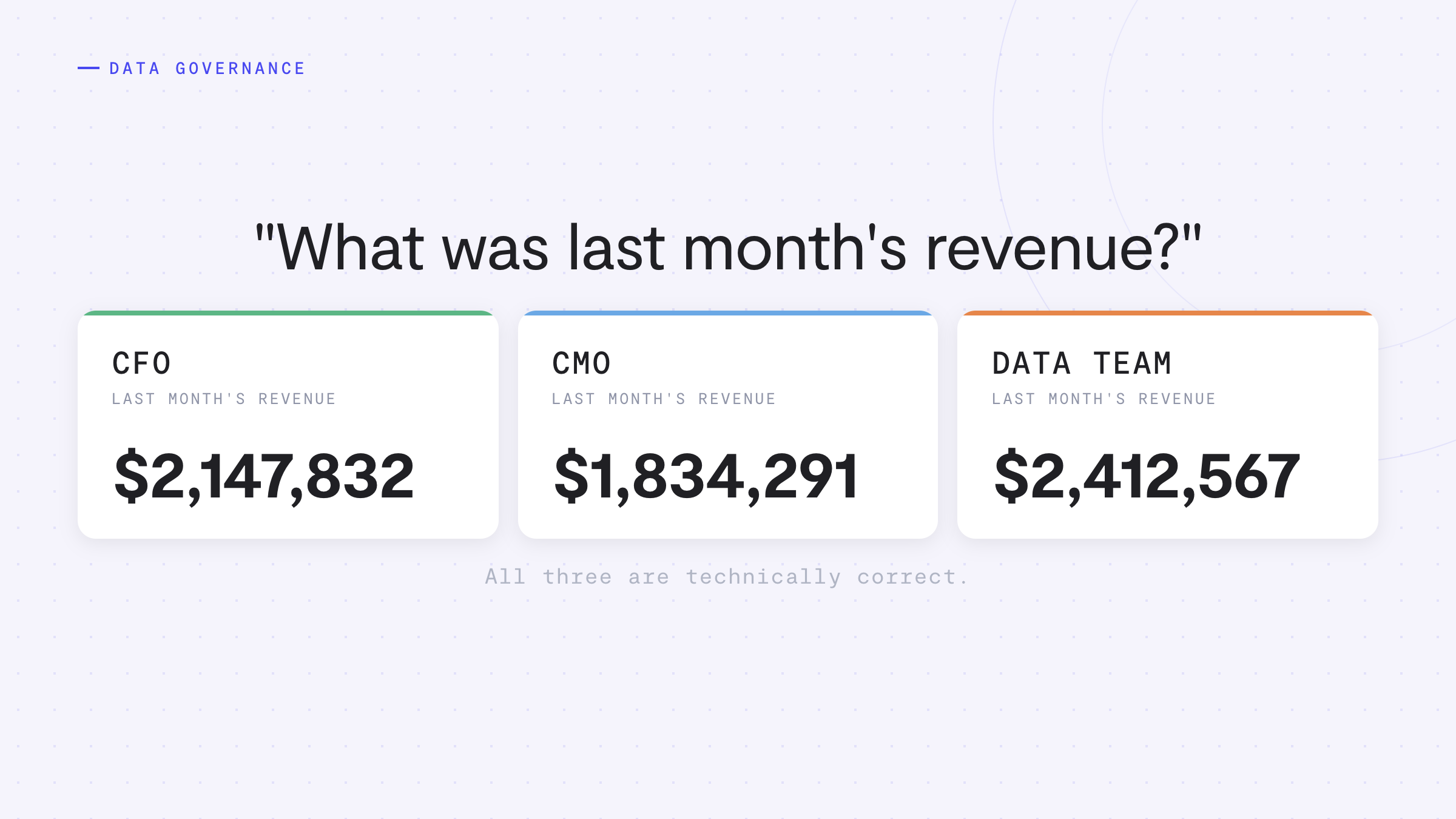
See where accuracy is won or lost across your data stack, and how a governed foundation changes the outcome.
Harness the power of AI without compromising on security.
A dedicated Technical Account Manager guides your team through it
Turn any dashboard into a clear, actionable summary in just one click
AI agents detect opportunities in your data and sync them across your platforms with our fully-managed Reverse ETL.
Sync data from 600+ sources, align KPIs, and see portfolio-wide results instantly.
Give every role the same board, filtered to exactly what they're allowed to see.
Help your clients become data driven faster through seamless reporting and collaboration tools.
Grow your census and strengthen your bottom line with HIPAA-compliant analytics.
AI-powered analytics for dental practices and DSOs. Track production, case acceptance, patient recare, and marketing ROI.
Turn data into success with complete visibility of every consumer interaction.
Make data-driven decisions that enhance patient care and your bottom line.
HIPAA-compliant AI agents that optimize operations, marketing, and patient care across every med spa location.
AI-powered analytics for plastic surgery practices. Track consult conversion, surgeon performance, and marketing ROI.
AI agents that monitor, analyze, and optimize performance across every portfolio company.
Easily surface the data you need to increase sales and drive revenue.
Measure every hospital the same way and track compliance across your whole group.
See how AMP scaled profitability and enhanced patient care
See how CorralData & Evolve Results built ADVENT a true ROI engine
See how AMNH gained a better understanding of the ‘why’ behind their data
See how BodyLase unlocked full data visibility, enabling smarter marketing and stronger results
See how evolvetogether used AI-powered insights to shape a unified growth strategy
See how Geode Health unlocked the value of their data while protecting patient privacy
See how Engine identified and converted more high-value customers
See how AI and unified data drove revenue growth at Inspire Aesthetics
See how Lacoste boosted their e-commerce performance with AI-driven insights
See how Moon Juice used live insights to find, reach, and convert their best customers
See how Olympus uses data and AI to fuel growth
See how Options Medical Weight Loss maximized their LTV:CAC
See how Pfizer turned complex data into real-time marketing intelligence
See how Ready Set Rocket streamlined client reporting and unlocked real-time insights
See how Solo Stove measures true channel ROAS with a marketing mix model in CorralData
See how St. John Knits increased marketing efficiency by 50%
See how sweetgreen acquired new customers and built stronger relationships with their most loyal patrons
CorralData | In partnership with Aviva Aesthetics
We recently joined Aviva Aesthetics for a live webinar with medspa operators on one of the most common growing pains in the industry: what happens to your data, your visibility, and your decision-making when you go from one location to many. We’ve turned the webinar into this article for anyone who couldn’t make it, or who wants a reference they can come back to.
– – – – –
At one location, most operators have a clear picture of their business. They know which providers are retaining patients, which marketing channels are working, and roughly what each service line is worth. Add a second location and that picture starts to blur. Add four and it’s gone. This is not a management problem. It is a data infrastructure problem, and it follows the same pattern across every practice that scales.
CorralData works with over 80 active multi-location medspa and aesthetics brands, representing more than 1,000 locations. What we see at onboarding, consistently, is the same set of four blind spots. They do not appear because operators are doing anything wrong. They appear because the data required to run a multi-location practice is scattered across three systems that were never designed to talk to each other. Until they do, the questions that matter most are unanswerable.
BY THE NUMBERS
9 in 10 multi-location operators cannot answer basic profitability questions before connecting their data
45% of average practice revenue has no attribution data at all during CorralData onboarding
34 pts retention gap observed between best and worst provider within the same portfolio
The four blind spots that follow are the gaps we diagnose at nearly every onboarding, whether a practice is at three locations or thirty. Each one is manageable at a single location. Each one compounds as you grow.
“You can’t coach what you can’t see.”
At a single location, you know your providers intuitively. You see who is fully booked, who patients ask for by name, and who has patients that quietly stop coming back. At two or three locations, that intuition disappears. You start looking at aggregate revenue numbers and completely miss that two providers in the same building have a 34-point gap in patient retention. That gap is not just a metric. It is a coaching problem, a scheduling problem, and a revenue problem, all at once.
Within a single multi-location group, we regularly see annual revenue per provider range from $32,000 to $183,000. That spread exists inside the same brand, often on the same EMR. The operators managing those practices frequently do not know it until their data is unified.
What operators need to track here:
“Total revenue hides everything.”
At one or two locations, most operators are focused on revenue growth. Open the next location, fill the book, grow the top line. That orientation makes sense early. But somewhere between locations two and four, a more important question emerges: which of these locations is actually profitable, and at what margin?
Most operators cannot answer this because financial data lives in QuickBooks or a similar accounting platform, and operational data lives in Zenoti, Meevo, or another EMR. Those systems have never been connected. The result is that expansion decisions get made on top-line revenue alone, without visibility into what each location actually costs to run or earns per service hour.
Most operators CAN see:
Most operators CANNOT see:
“You know what your channels cost. You don’t know what they’re worth.”
As practices grow, marketing spend grows with them. More locations mean more campaigns, more channels, more budget to justify. But the data that would tell you whether that spend is actually working is split across three systems: your EMR holds patient history and revenue, your analytics platform holds web behavior, and your ad platforms hold campaign performance. 45% of an average practice’s revenue has no attribution data at all when they first connect to CorralData. Nearly half their business is invisible to their marketing team.
The deeper problem is how ad platforms optimize. A campaign driving a low cost per appointment looks like a win. But if those appointments are showing up as no-shows at a higher rate, the real cost per kept appointment is far higher. Ad platforms cannot see inside your EMR. They optimize toward what they can measure, which is appointments booked, not revenue generated. Connecting your EMR data to your ad platforms is the only way to shift that optimization toward patients who actually show up and spend money.
Across the 80-plus multi-location brands we work with, 9 in 10 operators cannot answer three basic questions before connecting all of their data:
None of these are answerable from a single system.
“Your highest-value patients are the easiest to lose track of.”
Members are the highest-value patients in any medspa. They generate roughly $460 per month compared to $230 for non-members, and they visit approximately twice as often. That gap in lifetime value makes membership conversion and retention one of the most powerful financial levers in the business. It is also one of the most difficult to manage across locations.
At a single location, lapsed members are visible. At five or ten locations, they disappear into aggregate numbers. Which locations are converting memberships, which members are quietly lapsing, what the revenue impact of each lapse actually is, and how package expiration is tracking across locations: these questions require a cross-location view that most EMR platforms cannot provide without connecting to a unified reporting layer.
Not all metrics are equal. The operators who run the most successful multi-location practices tend to focus on a tightly defined set of KPIs they review consistently, rather than building expansive dashboards nobody opens. Based on the most frequently built reports and most common AI queries across our customer base, here is what top operators are actually tracking.
Financial
Operational
Retention and Marketing
This is consistently the most-built leaderboard widget across our customer base. It surfaces the productivity gap between providers at the same location and across locations, and it creates the kind of friendly competition that drives real performance improvement. One of our customers brought location-level rebooking rate comparisons to a board meeting and discovered that one practice was dramatically outperforming others. That practice shared their process. The insight only existed because the data was unified across locations.
Rebooking rate (and why the definition matters)
Every practice has a slightly different definition of rebooking rate. What matters less than which definition you use is that the same definition is applied consistently across all locations. When rebooking rate is calculated differently at each location, comparisons are meaningless, and the coaching and competitive value of the metric disappears.
90-day patient retention by location
This metric does double duty. As a retention signal it tells you where you are losing patients between visits. As a marketing tool, a list of patients outside the 90-day window can be sent back to your CRM in a HIPAA-compliant way for reactivation campaigns, and used to create optimized audiences in ad platforms so your campaigns find more people who look like your high-retention patients.
Patients without future appointments
Patients without future appointments is not a metric to monitor passively. It is a work queue. The practices that treat it as an automated report sent to location managers, who then call those patients, see retention move measurably. The ones that leave it on a dashboard do not.
It’s cheaper to retain a patient than to acquire one, no matter how many locations you have. The practices that grow most efficiently are the ones obsessed with retention, not just acquisition.
The data required to answer the questions above already exists. The problem is that it lives in three separate systems that weren’t designed to communicate with each other.
Your EMR holds the clinical and operational picture: appointments, services, provider output, patient treatment history, retention and rebooking. Your accounting software holds the financial picture: revenue by location, labor costs, cost of goods, margin by service. Your ad platforms and analytics tools hold the marketing picture: ad spend by channel, new patient acquisition, campaign performance, source attribution.
Only when all three are unified can you answer the question that actually changes how you run the business: which marketing channel brings patients who generate the most revenue over 12 months? That is the question that tells you how to allocate every dollar, not just in marketing, but in expansion decisions as well.
Beyond the four blind spots, there are four operational patterns that create problems for almost every operator scaling from a handful of locations to a dozen or more.
1. Two sources of truth
Your EMR reports one revenue number. Your finance team’s report shows another. When that happens repeatedly, confidence collapses and teams stop using dashboards. The fix is agreeing on metric definitions in advance, showing both calculations, and documenting clearly how the reporting version is derived. This sounds basic but almost no scaling practice has done it.
2. Service and provider naming inconsistency
We have not encountered a single roll-up or acquisition that did not have this problem. Each location calls services and treatments differently. Providers change their names, or their profiles get duplicated, and revenue appears to split across ghost records. The fix is a normalized service taxonomy applied consistently, with historical data unified under standardized labels.
3. New location ramp contamination
A new location looks terrible for its first 90 to 180 days. Blend it into your portfolio metrics without tagging it separately and everything looks like it is declining, when actually you are looking at a ramp period mixed with mature location performance. New locations need to be explicitly tagged and segmented from mature benchmarks from day one.
4. Goals that live in a spreadsheet
Goals set monthly and reviewed monthly mean nobody knows where they stand in the middle of the month. Location managers cannot course-correct on what they cannot see in real time. Live distance-to-goal by location, visible daily to the people who can act on it, is one of the highest-impact operational changes a scaling practice can make.
The questions below are easy to answer with a single location. They become significantly harder, and eventually impossible, without unified data infrastructure.
CEO / Owner
COO / Operations
Marketing Lead
Practice Manager
A Note on Valuation
For operators building toward a PE exit or platform acquisition, data infrastructure is not just an operational consideration. It is a valuation factor. When an investor evaluates two practices of similar size, they will favor the one where location-by-location performance is transparent, KPIs are consistently defined across the portfolio, and financial and clinical data tells a coherent story.
Inconsistent service naming, disconnected financial and operational systems, and an inability to answer basic profitability questions by location are not neutral. They reduce confidence in the business and, ultimately, reduce multiples. The best mindset for any operator building toward scale: run your business as if it were always for sale. Not because you are selling, but because the operational discipline required to support that standard is the same discipline that makes the business compound.
Ready to see the full picture?
CorralData connects your clinical, financial, and marketing data in one place so you can stop guessing and start compounding. Click here to book a demo and see CorralData in action.

CorralData


Make your data work for you. Book a demo today to see CorralData in action.

